Menu
How to Capture Explicit Consent from Doctors at Scale ?

Capturing explicit consent from doctors has become one of the most difficult operational challenges for pharma marketing teams under the Digital Personal Data Protection Act 2023. While the requirement itself is clear, the execution is not. Most existing systems, workflows, and engagement models were never designed to capture consent in a way that is explicit, purpose specific, auditable, and scalable.
Yet scale is unavoidable in pharma marketing. Engagement programs often involve thousands of doctors across geographies, specialties, and channels. Expecting manual consent collection or fragmented approaches is unrealistic.
This is where many teams struggle. They understand the legal requirement but cannot translate it into operational reality. This article explains how pharma companies can capture explicit consent from doctors at scale, without slowing down engagement or creating unmanageable complexity.
Why Explicit Consent at Scale Is a Pharma Specific Problem ?
In most industries, consent capture happens at the point of customer onboarding. In pharma, doctor engagement is continuous and multi layered.
Doctors interact with pharma companies through field representatives, conferences, digital platforms, webinars, email campaigns, WhatsApp messages, and educational portals. Consent may be captured in one context and reused in another.
Under DPDP, this reuse becomes risky unless consent is explicit and purpose bound.
The challenge is not capturing consent once. The challenge is capturing it consistently, clearly, and at scale across multiple touchpoints.
What Explicit Consent Actually Requires Under DPDP ?
Before discussing scale, it is important to clarify what explicit consent means in practice.
Explicit consent requires a clear affirmative action by the doctor. The doctor must understand what data is being collected, why it is being collected, how it will be used, and through which channels communication will occur.
Consent must be specific to a purpose. It cannot be vague or open ended. It must also be recorded and capable of being withdrawn easily.
Any scalable consent model must satisfy all of these conditions.
Why Legacy Consent Collection Methods Fail at Scale ?
Many pharma companies attempt to retrofit explicit consent into legacy workflows. This often fails.
Paper forms collected by field teams do not scale well and are difficult to audit. Email based consent requests are ignored or lost. Consent captured during conferences is often broad and poorly documented.
Most critically, these methods do not integrate well with digital systems. Consent remains disconnected from execution.
At scale, disconnected consent is almost worse than no consent, because it creates false confidence.
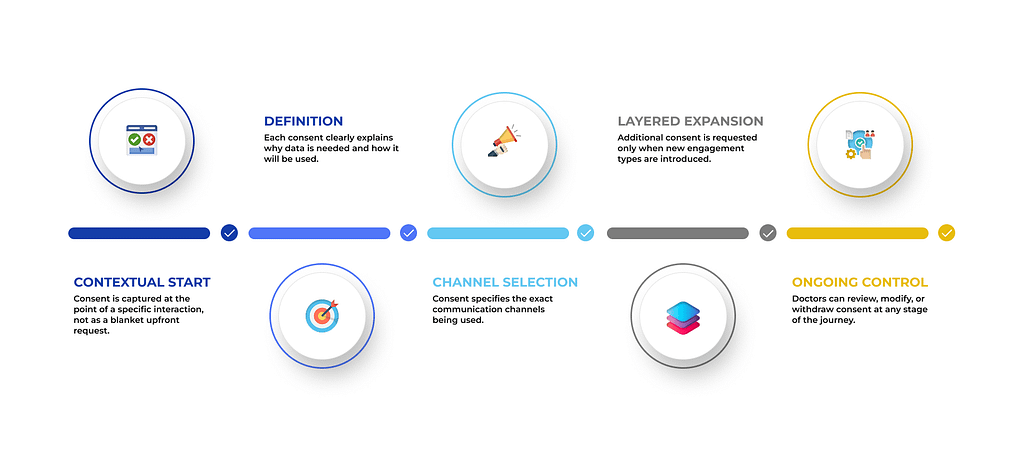
Designing Consent as a Journey, Not an Event
One of the biggest shifts required under DPDP is moving from event based consent to journey based consent.
Doctors should not be asked to give blanket consent upfront for all future engagement. Instead, consent should be captured contextually, aligned to specific engagement journeys.
For example, a doctor attending a digital education program may be asked for consent specific to educational communication. A separate consent may be requested later for promotional updates.
This layered approach allows consent to grow naturally while remaining explicit and defensible.
Using Digital Touchpoints to Capture Consent at Scale
Digital touchpoints are the most scalable channels for consent capture.
Doctor portals, webinar registrations, mobile applications, and content platforms provide natural moments to present clear consent requests. These interfaces allow consent language to be standardised and logged automatically.
The key is to ensure that consent requests are simple, unambiguous, and directly tied to the activity the doctor is engaging in.
Overly legal language reduces acceptance. Clear, professional language increases trust.
Integrating Consent Capture with Field Force Workflows
Field teams remain central to doctor engagement. Ignoring them in consent strategy is a mistake.
However, field force consent capture must be digitised. Mobile tools used by representatives should include consent capture modules that record explicit consent in real time.
Consent captured during field interactions should flow directly into central systems. Manual handoffs or delayed uploads undermine auditability.
Training field teams to explain consent clearly is as important as the technology itself.
Centralising Consent Management
Scale requires centralisation.
Consent captured across channels must be stored in a central consent repository. This repository should map consent to doctor identity, purpose, channel, and timestamp.
Centralisation ensures that consent is enforced consistently across CRMs, marketing platforms, and analytics systems.
Without centralisation, scale multiplies risk rather than control.
This is where DPDP-compliant HCP marketing architectures become critical, because they treat consent as a shared operational signal rather than a siloed record.
Making Consent Enforcement Automatic
Capturing consent at scale is only half the problem. Enforcing it is equally important.
Systems must automatically check consent before outreach. Campaign automation should not rely on manual filters or assumptions.
If consent is missing or withdrawn, execution must stop without human intervention. This requires tight integration between consent systems and engagement platforms.
Automation reduces human error and supports scale.
Handling Consent Withdrawal at Scale
DPDP requires that consent withdrawal be easy and respected.
At scale, withdrawal handling must be automated. Doctors should be able to withdraw consent through digital channels without friction. Withdrawal must propagate across all systems and partners.
Manual processes do not scale here. Delays increase risk.
A scalable consent model treats withdrawal as a first class event, not an exception.
Managing Consent Across Multiple Purposes
Doctors often engage with pharma companies for multiple reasons.
They may participate in educational programs, receive scientific updates, and engage in promotional communication. Each purpose requires distinct consent.
Scalable systems must support multiple consent types per doctor. Treating consent as a single yes or no flag is insufficient.
Purpose based consent models allow engagement to remain compliant while still flexible.
Addressing Legacy Databases
Most pharma companies already hold large doctor databases.
Capturing explicit consent at scale does not mean discarding this data. It means revalidating it systematically.
Legacy doctors can be migrated into new consent journeys. Consent can be refreshed through digital campaigns, portals, or field interactions.
This transition must be planned carefully to avoid disruption.
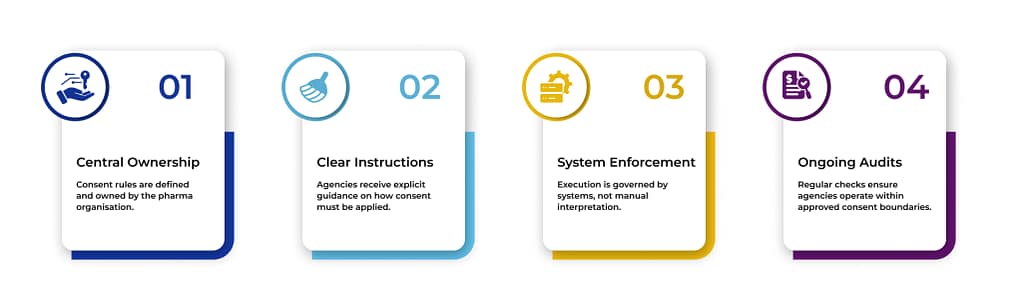
Aligning Agencies and Vendors to Consent Strategy
Agencies and vendors must operate within the consent framework defined by the pharma company.
At scale, this requires clear instructions, system level enforcement, and regular audits. Agencies should not manage consent independently.
Central ownership reduces fragmentation and risk.
Measuring Consent Health as a Metric
At scale, consent becomes a measurable asset.
Pharma companies should track consent coverage by purpose and channel. Gaps should be visible. Consent refresh rates should be monitored.
This turns consent from a compliance obligation into an operational metric.
Why Explicit Consent at Scale Improves Engagement Quality ?
While explicit consent may initially reduce the size of reachable audiences, it improves quality.
Doctors who provide explicit consent are more engaged, less likely to complain, and more receptive to communication. Trust improves.
Over time, this leads to better outcomes despite lower raw volumes.
Frequently Asked Questions on Capturing Explicit Consent at Scale
What does explicit consent mean under DPDP Act?
⌄
It means clear, informed, purpose specific permission given by the doctor for data use.
Can explicit consent be captured digitally?
⌄
Yes. Digital channels are the most scalable way to capture explicit consent.
Is field force consent capture allowed under DPDP?
⌄
Yes, if consent is recorded digitally and stored centrally.
Does consent need to be captured for each purpose?
⌄
Yes. Consent must be purpose specific.
Can old consent records be reused?
⌄
Only if they meet DPDP requirements for clarity and auditability.
How should consent withdrawal be handled at scale?
⌄
Through automated processes that propagate across all systems.
Do CRMs support explicit consent models?
⌄
Most require enhancements or integration to support DPDP level consent.
Who is responsible for consent enforcement?
⌄
The pharma company, as the data fiduciary, remains responsible.
Closing Perspective and CTA
Capturing explicit consent from doctors at scale is not a one time project. It is a capability that must be built into pharma marketing operations.
Teams that invest in consent first design, centralised systems, and automated enforcement will be able to scale engagement confidently under DPDP.
If you are evaluating how to implement DPDP-compliant HCP marketing with explicit consent capture at scale, this page explains how consent-first engagement models are being operationalised in real pharma environments.