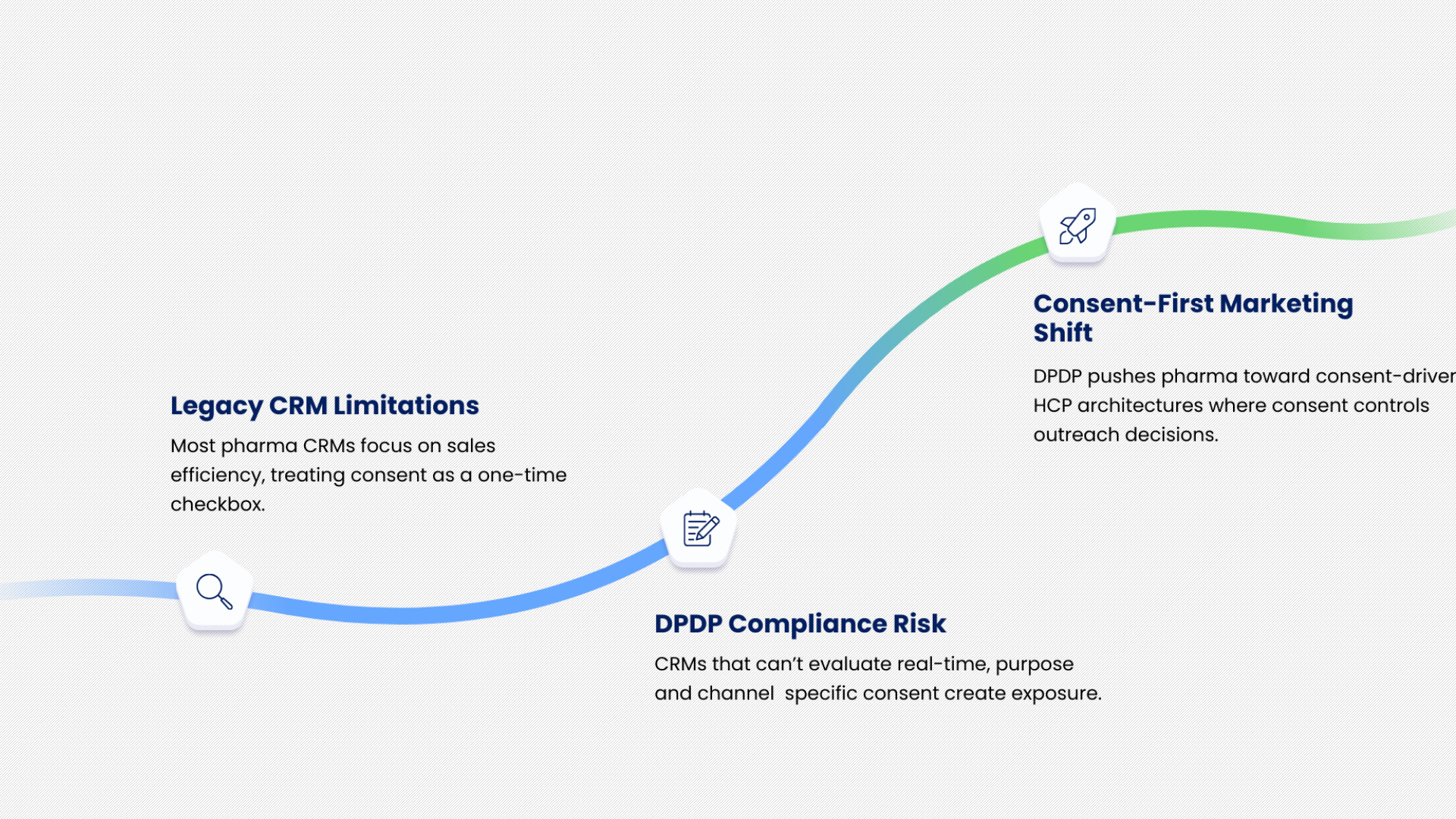
Many pharma CRMs were designed to optimise sales force productivity and campaign reach. Consent, if captured, was often treated as a compliance checkbox rather than an operational control. DPDP exposes this limitation.
A CRM that cannot dynamically evaluate consent at the moment of outreach creates risk.
A CRM that cannot map consent to specific purposes or channels cannot support DPDP-compliant execution. This is why DPDP pushes pharma marketing toward consent-first HCP marketing architectures, where consent intelligence is embedded into campaign decisioning rather than layered on top.
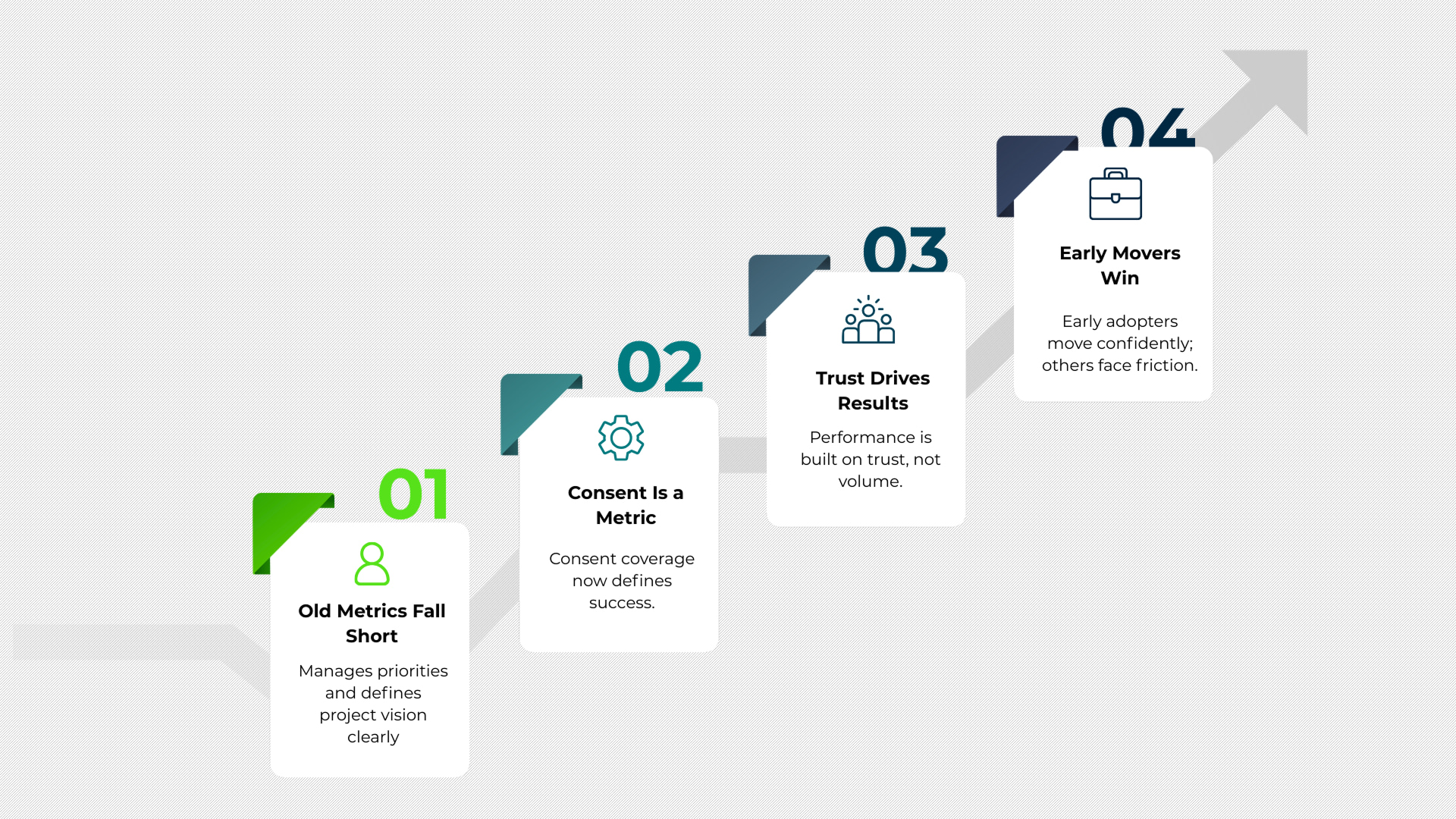
Traditional marketing metrics focused on reach, opens, clicks, and frequency. DPDP introduces a new dimension that cannot be ignored.
Consent coverage becomes a critical metric. Auditability becomes a requirement. Data lineage matters as much as campaign performance.
This shifts success from volume driven metrics to trust driven execution.
Teams that adapt early will find it easier to operate confidently. Teams that delay will face increasing friction as audits, partner scrutiny, and regulatory expectations rise.