 Pharma systems evolved in silos.
Pharma systems evolved in silos.
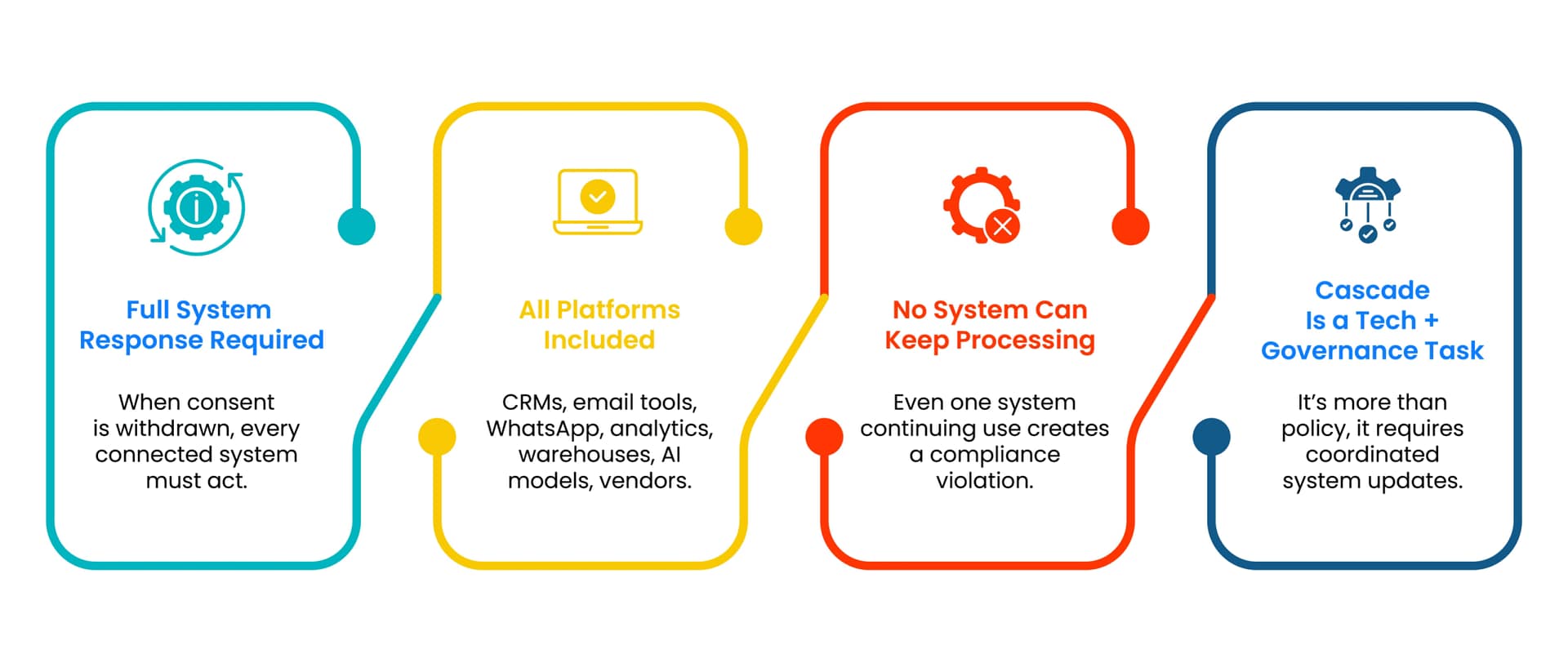
Email tools handle unsubscribes. WhatsApp platforms handle opt outs. CRMs store flags. Analytics tools continue to process historical data. Vendors retain copies.
These systems rarely communicate effectively.
As a result, consent withdrawal is handled inconsistently. Outreach may stop in one channel but continue in another. Analytics may still process data long after consent is withdrawn.
Under DPDP, this fragmentation is non compliant.
 Channel level opt outs address only one symptom.
Channel level opt outs address only one symptom.
Unsubscribing from email stops email delivery but does not stop WhatsApp messaging, ad targeting, analytics processing, or data sharing.
DPDP does not recognise channel level compliance as sufficient if processing continues elsewhere.
Consent withdrawal must be enforced across all channels and uses for that purpose.