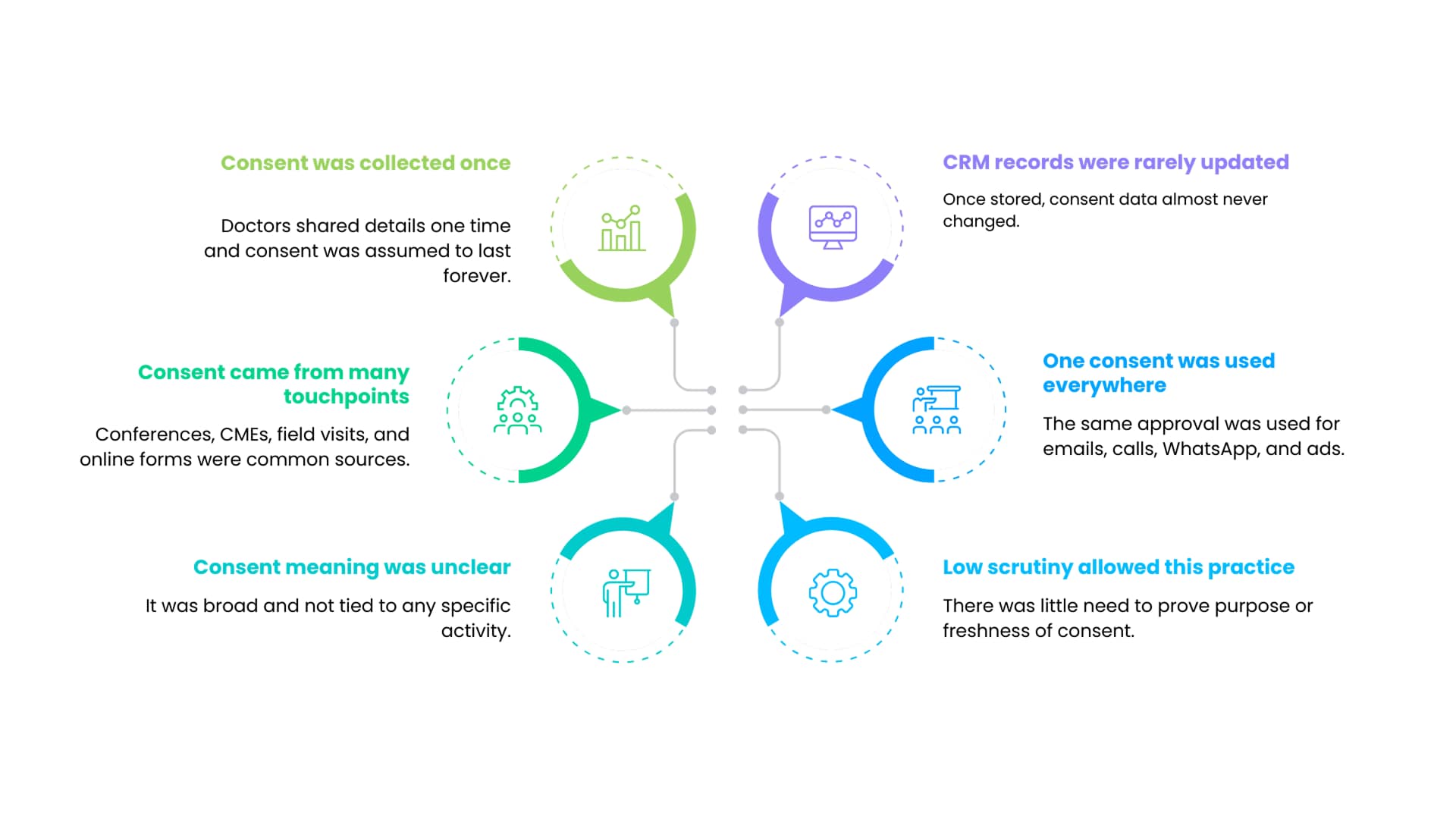
Historically, consent in pharma marketing was often captured once and reused many times. Doctors provided contact details during conferences, CME programs, field force interactions, or online registrations. That consent was usually broad and loosely defined.
Once stored in a CRM, the consent record rarely changed. It was assumed to apply to email, phone calls, WhatsApp messages, digital ads, and future campaigns that had not yet been designed.
This model worked largely because regulatory scrutiny around digital data use was limited. There was little requirement to prove purpose alignment or consent freshness.
DPDP invalidates this approach.
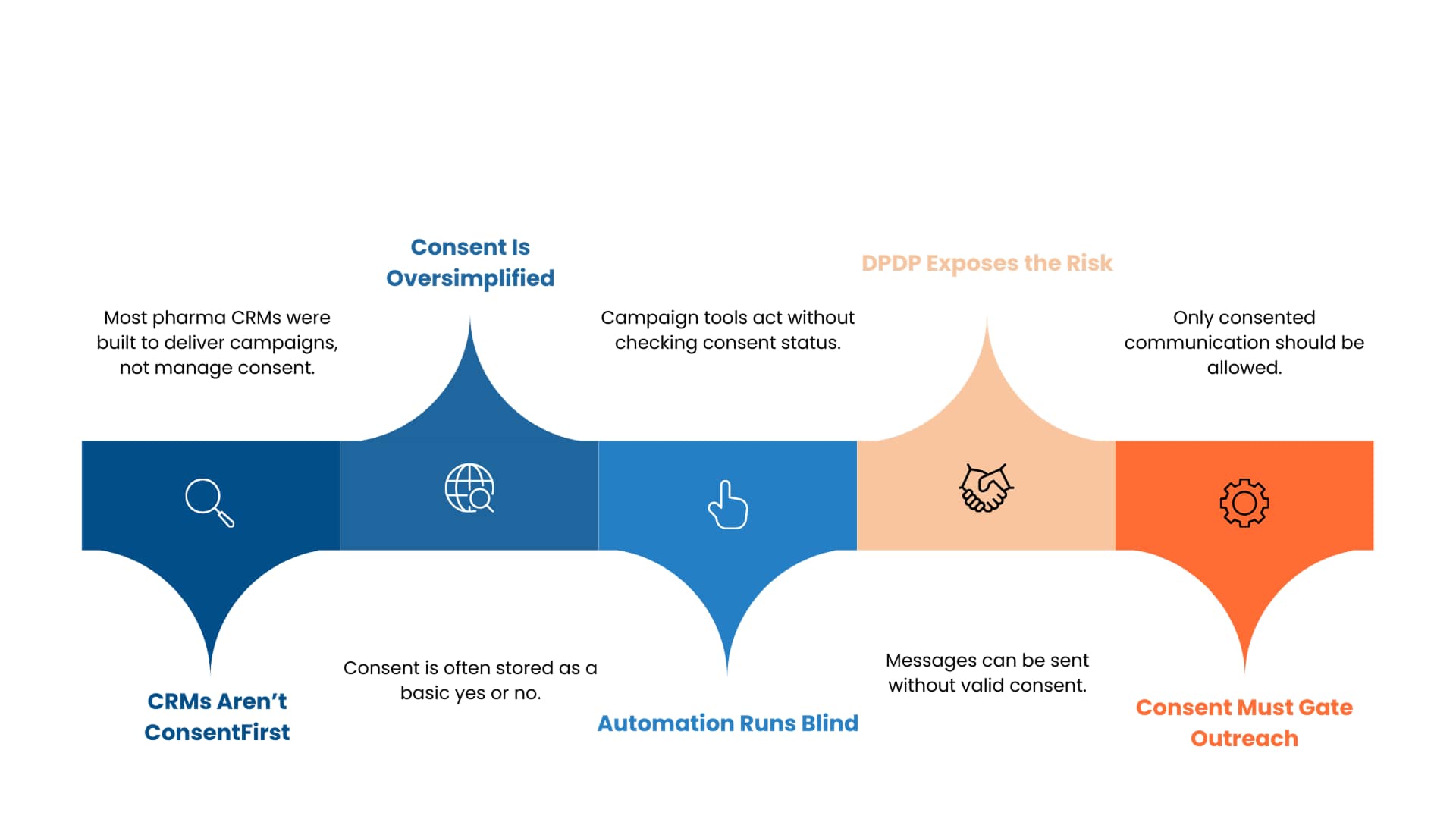
Most pharma CRMs were designed to optimise segmentation and campaign delivery, not to enforce consent logic dynamically.
Consent is often stored as a simple yes or no field, without purpose mapping or withdrawal workflows. Campaign automation tools then operate independently of consent context.
Under DPDP, this separation creates risk. Marketing automation must be consent aware. Outreach must be blocked automatically where consent does not exist.
This is where DPDP-compliant HCP marketing architectures become essential, because they integrate consent enforcement directly into campaign execution.