 Data minimisation under DPDP means limiting personal data collection to what is necessary to achieve a defined and lawful purpose.
Data minimisation under DPDP means limiting personal data collection to what is necessary to achieve a defined and lawful purpose.
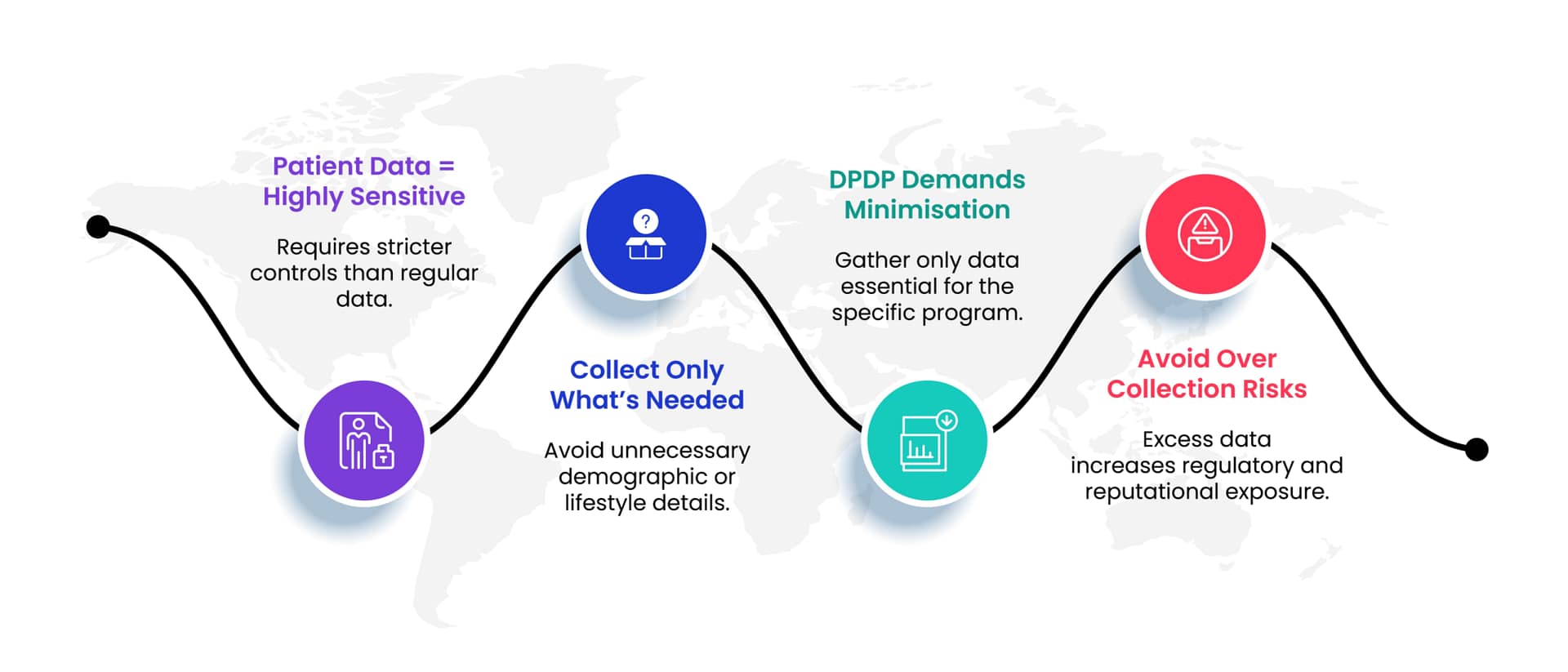
It is not about collecting less data arbitrarily. It is about collecting the right data with clear justification.
If a piece of data does not directly support a stated purpose, its collection and retention must be questioned. This applies equally to new data collection and to legacy data already stored.
For pharma companies, this principle affects doctor databases, patient programs, analytics platforms, and AI systems.
 Doctor data is one of the most heavily collected datasets in pharma.
Doctor data is one of the most heavily collected datasets in pharma.
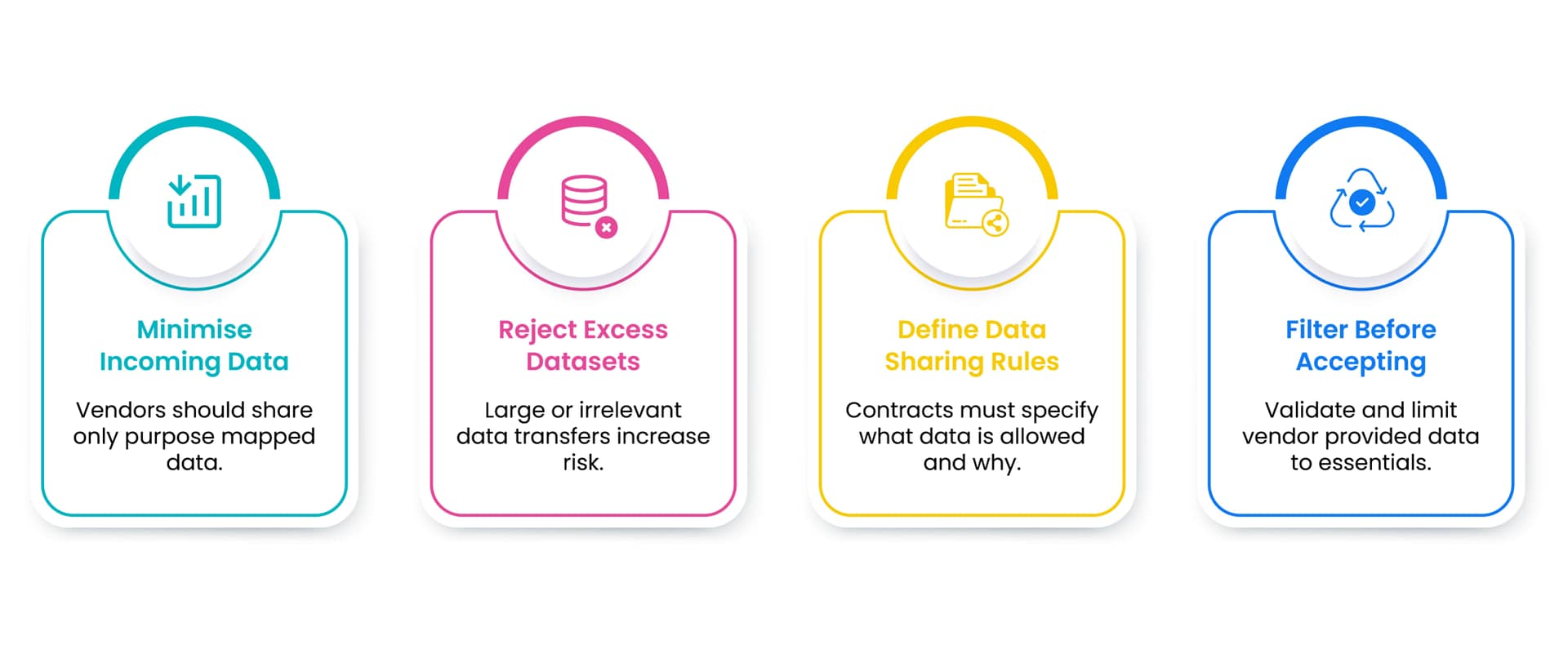
Beyond basic contact details, many databases include personal phone numbers, personal email addresses, social media handles, family details, travel preferences, behavioural scores, and inferred interests.
Much of this data is not necessary for compliant engagement.
Under DPDP, collecting data without a clear purpose creates risk. It increases the surface area for misuse, breaches, and audit findings.
Data minimisation requires pharma companies to question whether each data element is truly required.