What is DPDP Act 2023 in simple terms?
⌄
DPDP Act 2023 is India’s law that regulates how digital personal data can be collected, stored, processed, and used, including data used for pharma marketing and doctor engagement.
Does DPDP Act apply to pharma marketing teams?
⌄
Yes. Pharma marketing teams process doctor and patient data digitally, which brings their activities directly under the DPDP Act.
Is doctor data considered personal data under DPDP Act?
⌄
Yes. Doctor names, phone numbers, email IDs, clinic details, and engagement history qualify as personal data if they can identify an individual.
Can pharma companies market to doctors under DPDP Act?
⌄
Yes. DPDP does not ban doctor marketing, but it requires explicit, purpose-specific consent and compliant data handling practices.
Is consent mandatory under DPDP for doctor marketing?
⌄
Yes. Explicit consent is required before using doctor data for marketing, communication, or engagement activities.
What is explicit consent under DPDP Act?
⌄
Explicit consent means a clear, informed, and affirmative agreement by the doctor for a specific purpose, with the ability to withdraw consent at any time.
Is opt-in consent enough under DPDP Act?
⌄
In most cases, no. Generic opt-in consent without purpose clarity or auditability does not meet DPDP requirements.
Does DPDP Act affect existing doctor databases?
⌄
Yes. Existing databases must be reviewed to ensure lawful collection, valid consent, and purpose alignment. Legacy data is not automatically compliant.
Who is responsible for DPDP compliance in pharma marketing?
⌄
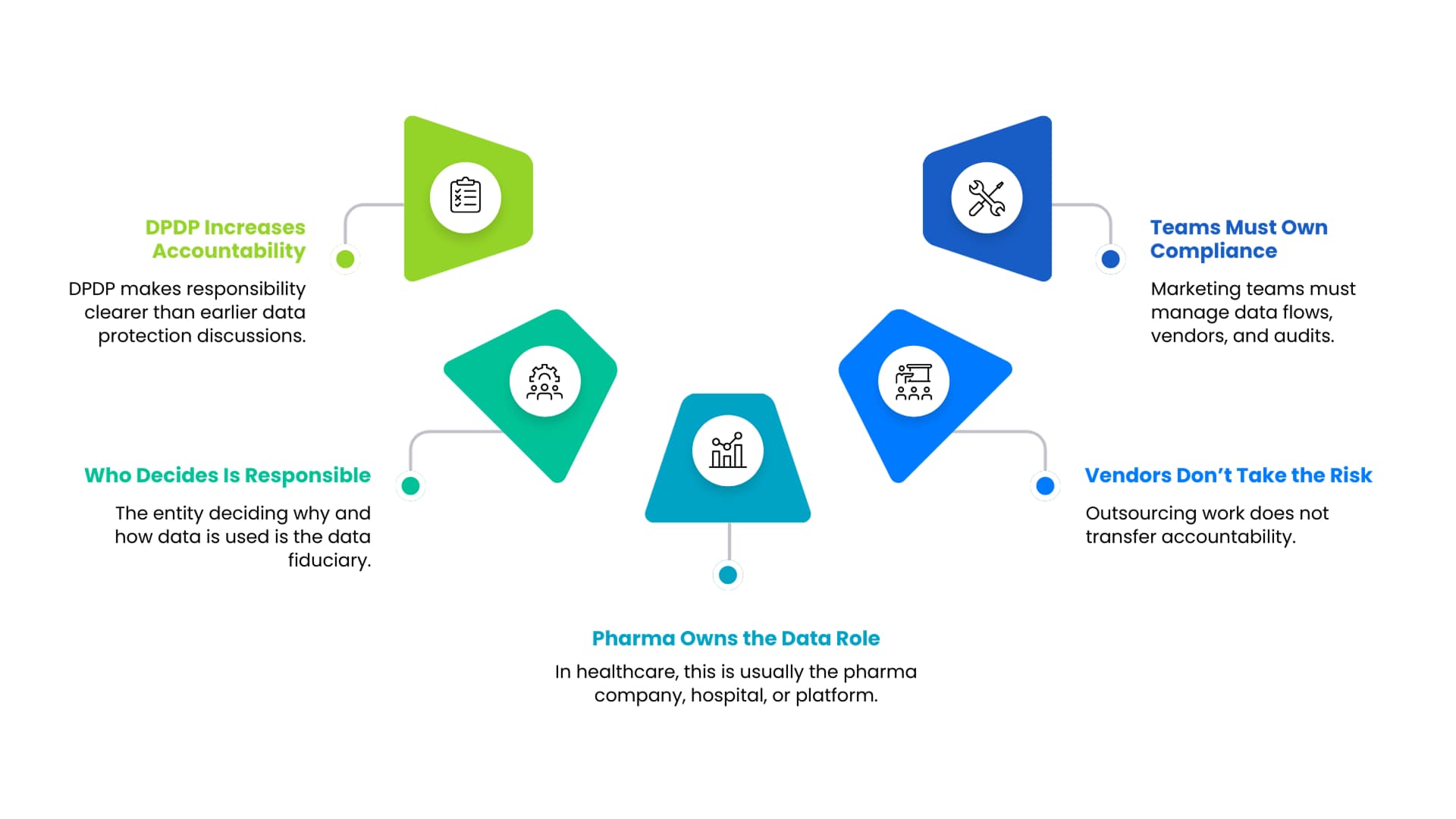
The pharma company is responsible as the data fiduciary, even if agencies, vendors, or CRM platforms are involved.
Can pharma companies still use WhatsApp and email marketing under DPDP?
⌄
Yes, but only if explicit consent exists for the specific channel and purpose of communication.
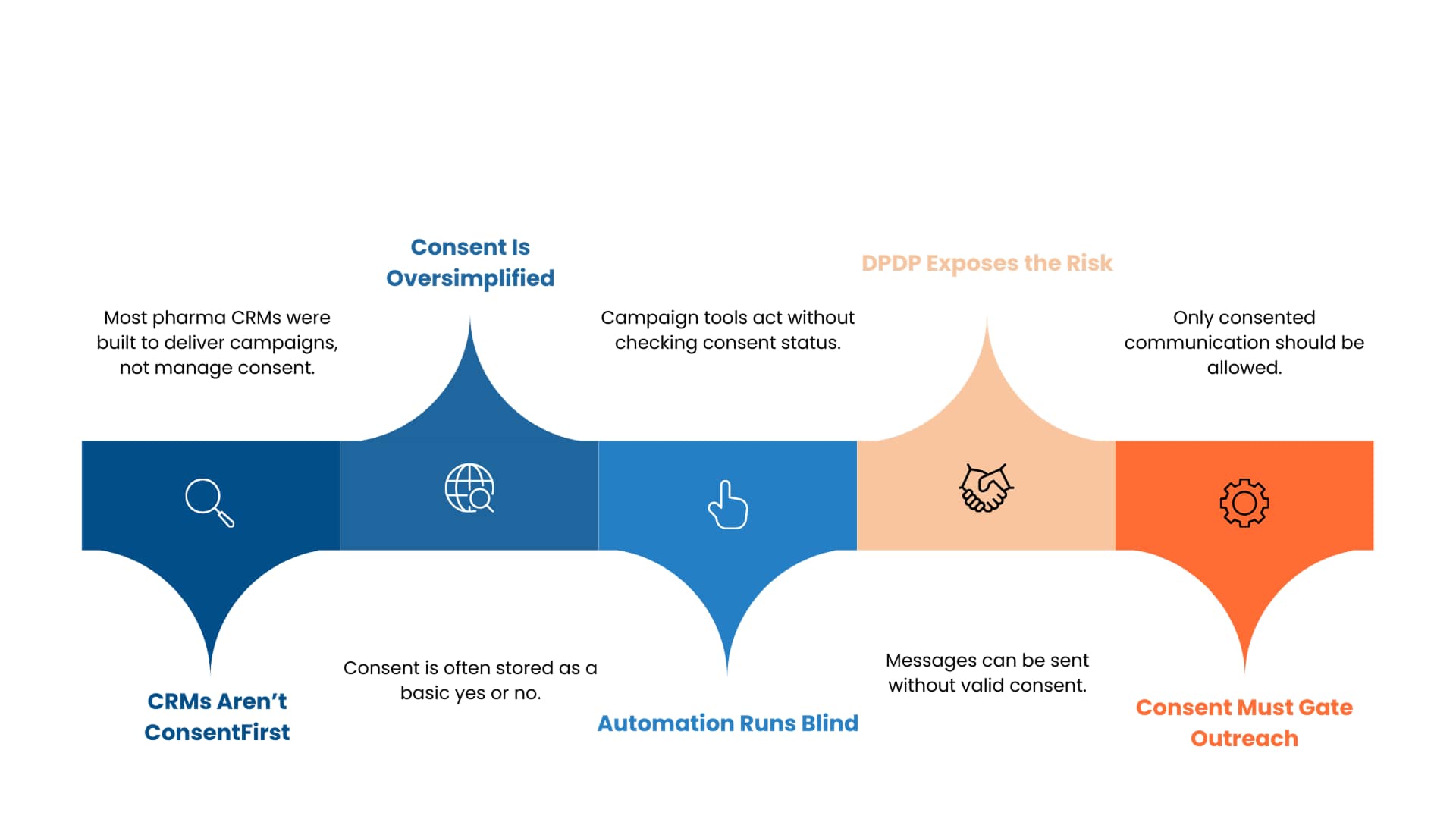
Does DPDP Act impact pharma CRM systems?
⌄
Yes. CRMs must support consent tracking, purpose mapping, and consent enforcement to avoid compliance gaps.
Are marketing agencies liable under DPDP Act?
⌄
Agencies act as data processors, but primary liability remains with the pharma company that determines how and why data is used.
What happens if consent is withdrawn by a doctor?
⌄
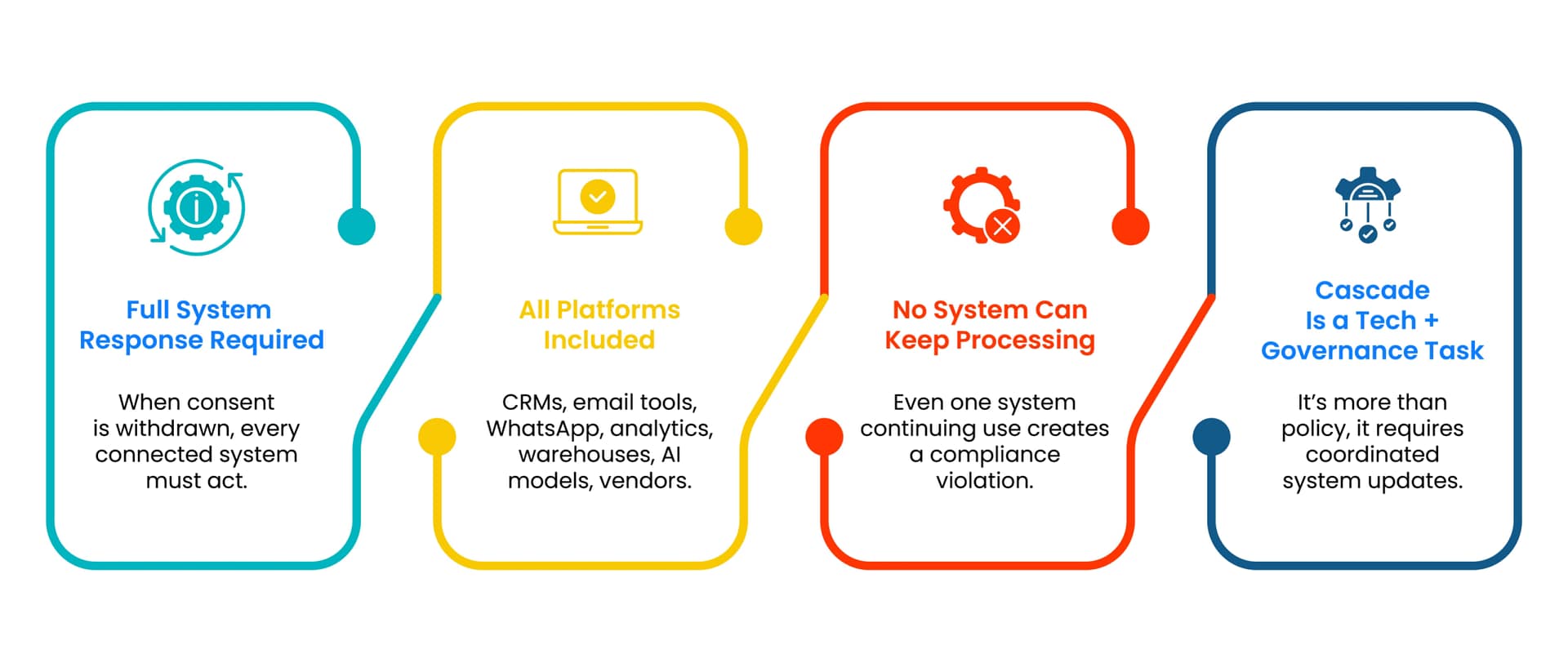
Once consent is withdrawn, the pharma company must stop processing the data for that purpose across all systems and channels.
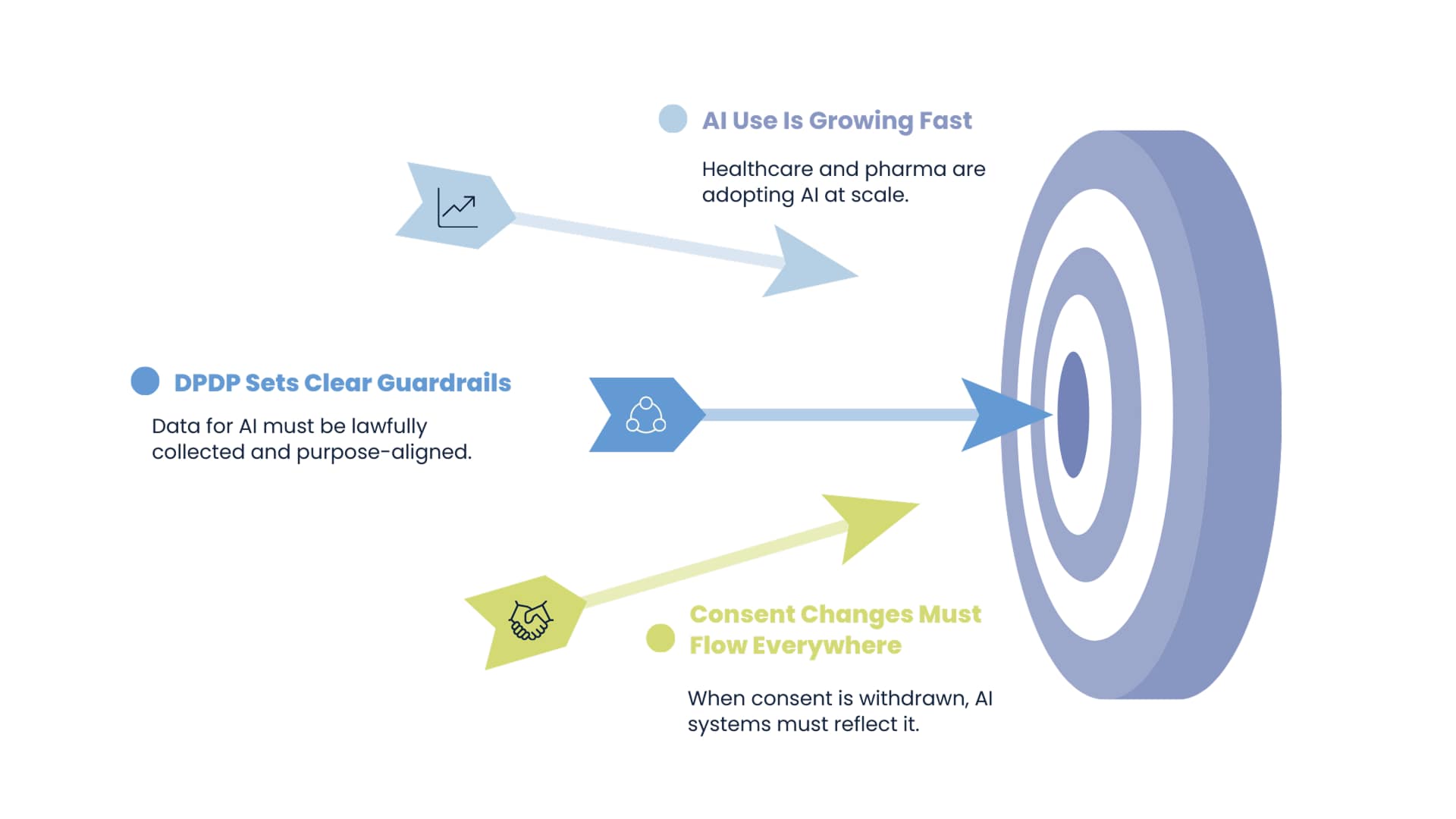
Does DPDP Act apply to AI-driven pharma marketing?
⌄
Yes. AI models using doctor data must comply with DPDP requirements, including lawful data use, consent scope, and purpose limitation.
What are the risks of DPDP non-compliance for pharma marketing teams?
⌄
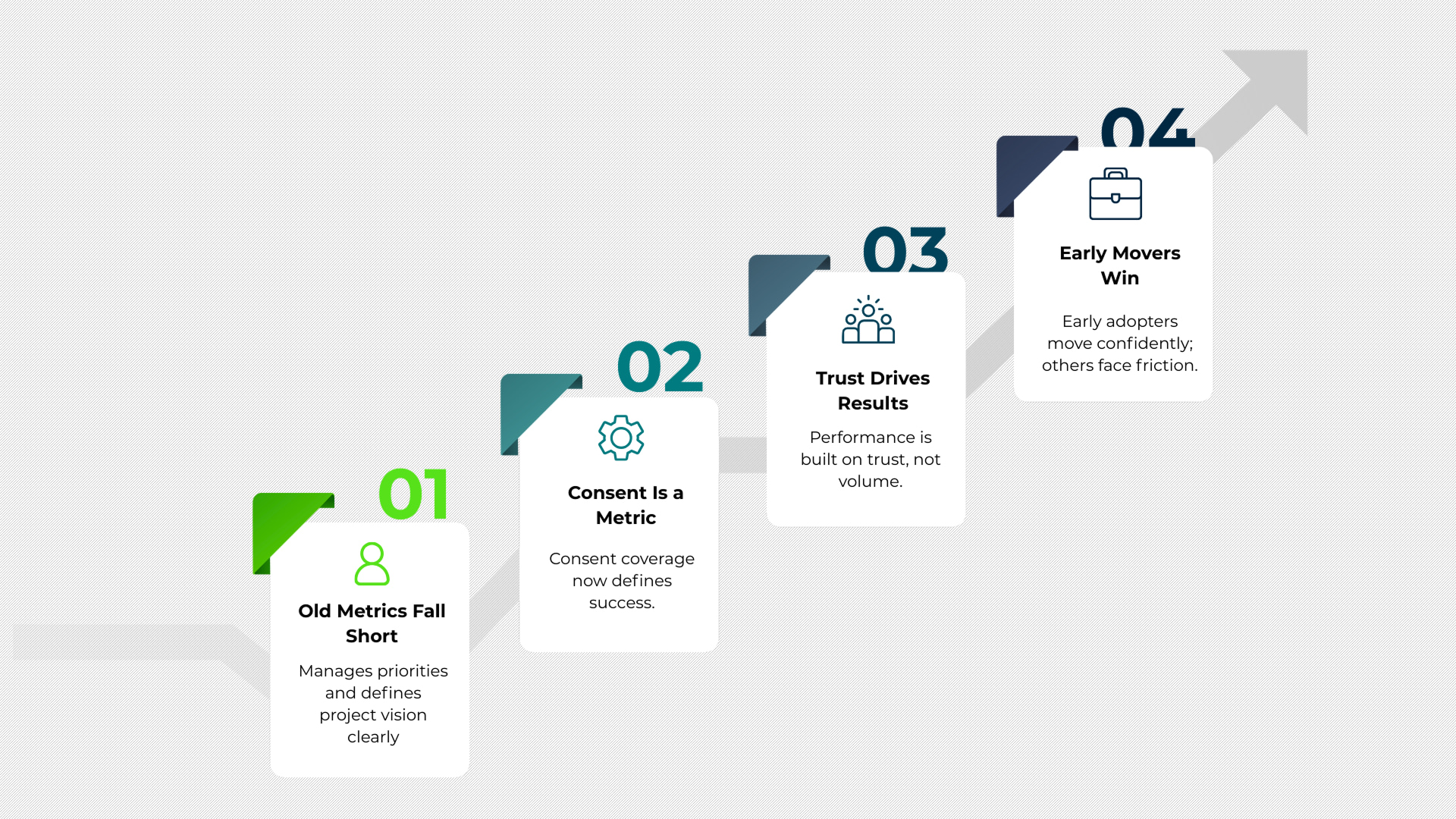
Risks include penalties, audits, campaign disruption, reputational damage, and loss of trust with doctors.

 Ignoring data fiduciary responsibilities does not eliminate liability. It increases risk.
Ignoring data fiduciary responsibilities does not eliminate liability. It increases risk.

![Why Pre-DPDP Consent Models No Longer Work in Pharma – [Cloned #21157]](https://mlmsgzbi9bun.i.optimole.com/cb:nQAU.8b/w:1920/h:1080/q:mauto/f:best/https://multiplierai.co/wp-content/uploads/2026/02/Why-Pre-DPDP-Consent-Models-No-Longer-Work-in-Pharma.png)


 At its core, the DPDP Act governs how digital personal data can be processed. Processing includes collection, storage, sharing, analysis, and use.
At its core, the DPDP Act governs how digital personal data can be processed. Processing includes collection, storage, sharing, analysis, and use.


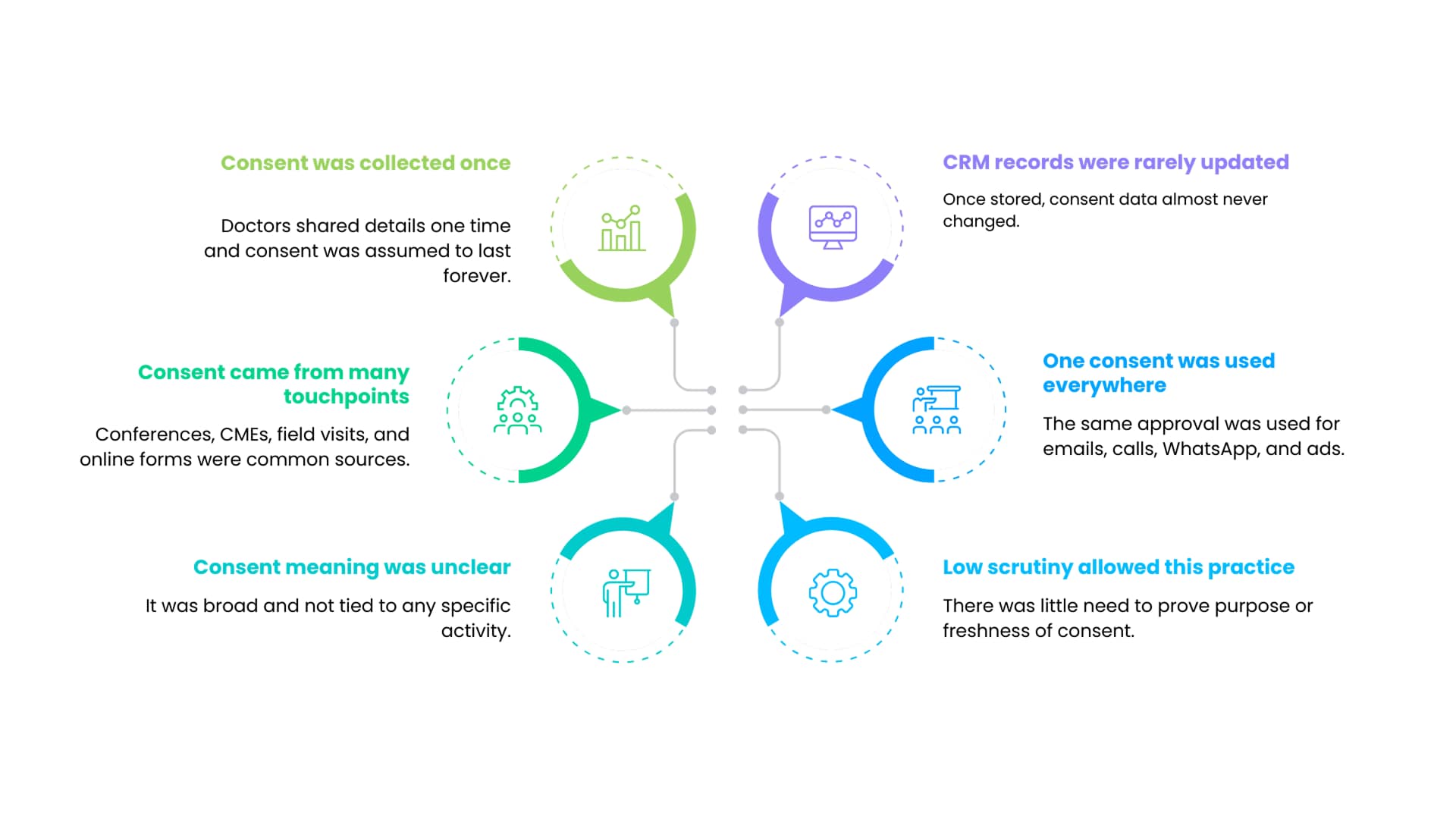
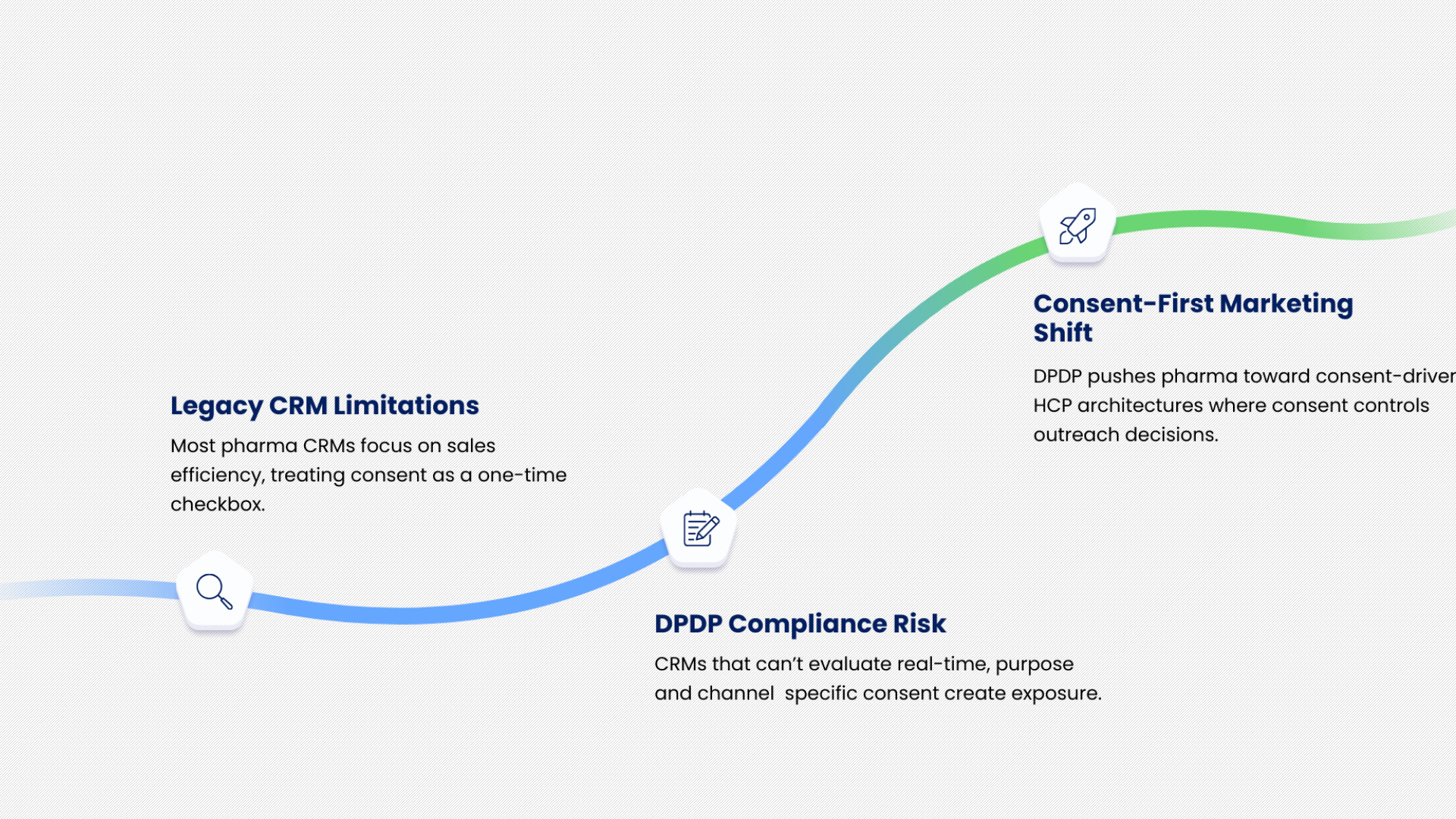
 Many pharma companies rely on historical consent to justify reuse.
Many pharma companies rely on historical consent to justify reuse. Purpose limitation is difficult because it requires clarity and discipline.
Purpose limitation is difficult because it requires clarity and discipline.
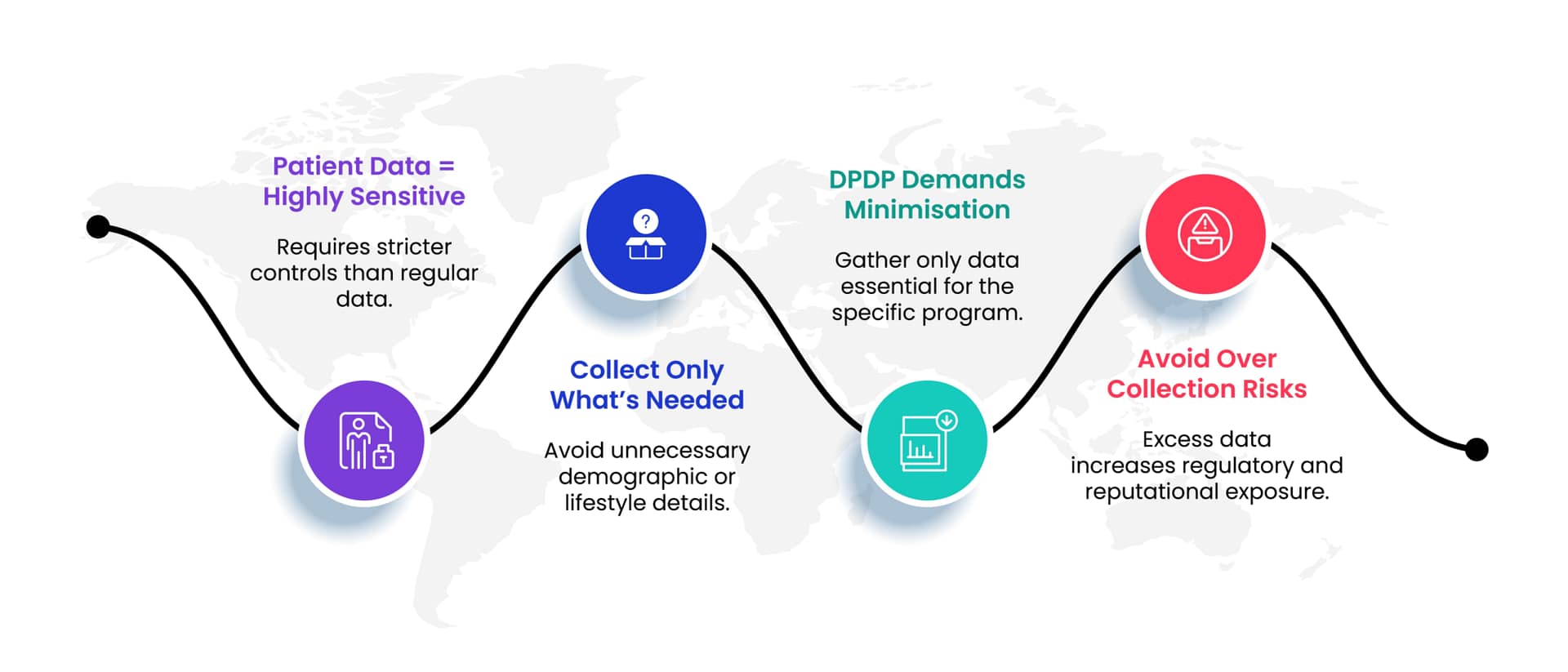 Data minimisation under DPDP means limiting personal data collection to what is necessary to achieve a defined and lawful purpose.
Data minimisation under DPDP means limiting personal data collection to what is necessary to achieve a defined and lawful purpose.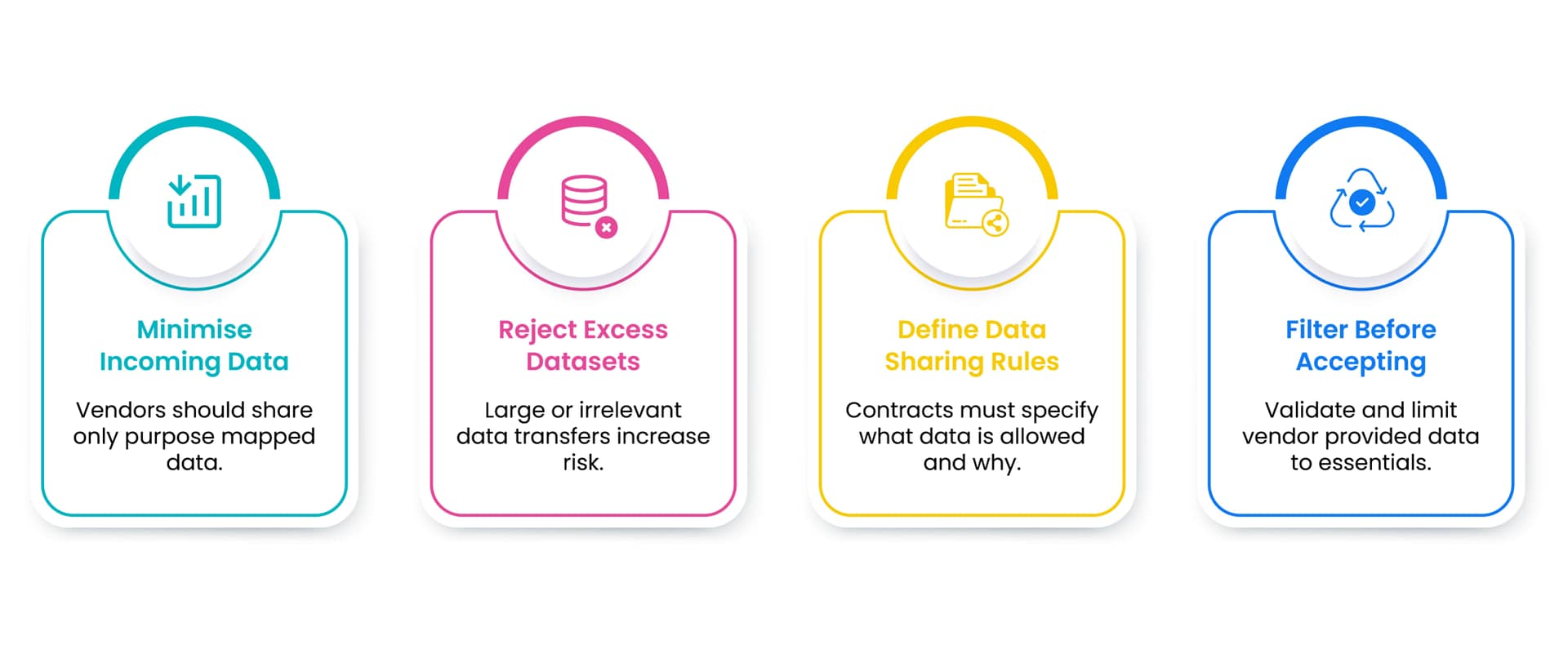 Doctor data is one of the most heavily collected datasets in pharma.
Doctor data is one of the most heavily collected datasets in pharma.

 A common misconception is that vendors are responsible for compliance failures involving their systems.
A common misconception is that vendors are responsible for compliance failures involving their systems.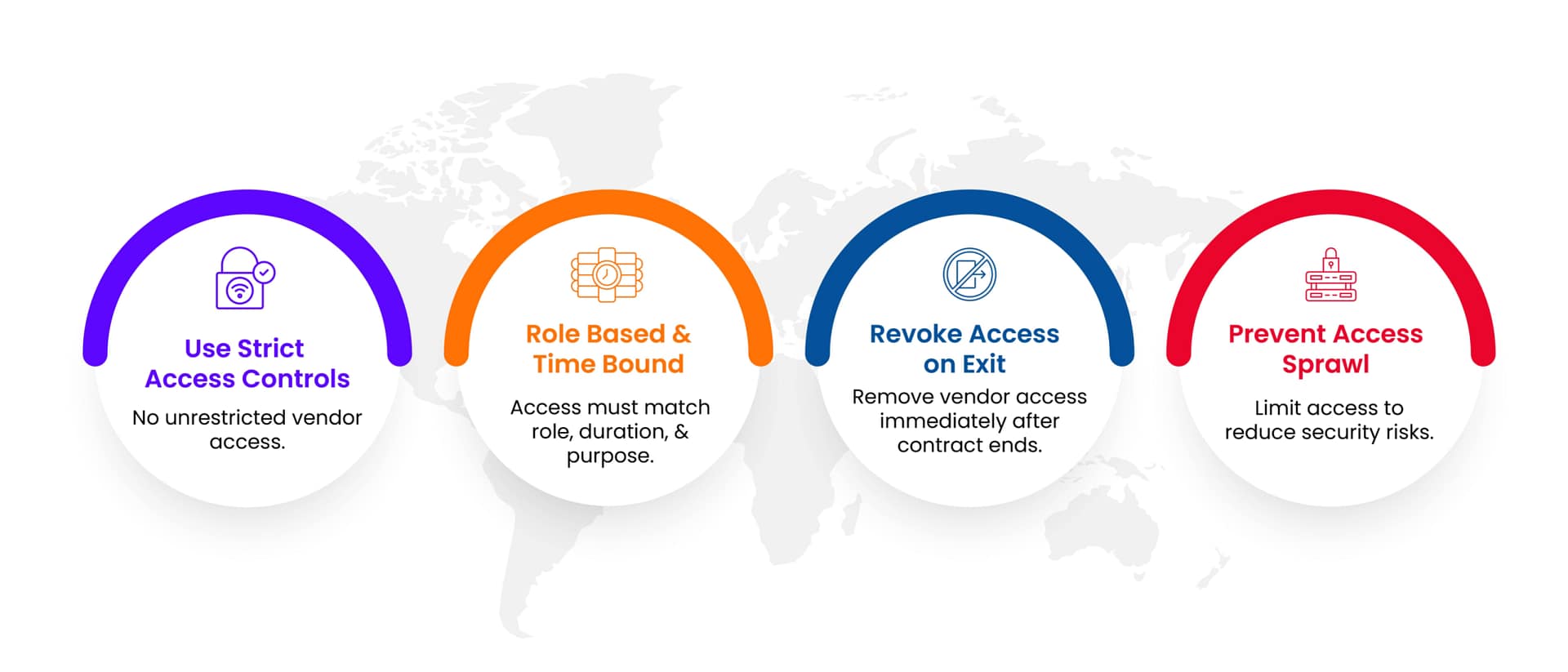 Vendor related DPDP risk is systemic.
Vendor related DPDP risk is systemic.
 Pharma systems evolved in silos.
Pharma systems evolved in silos.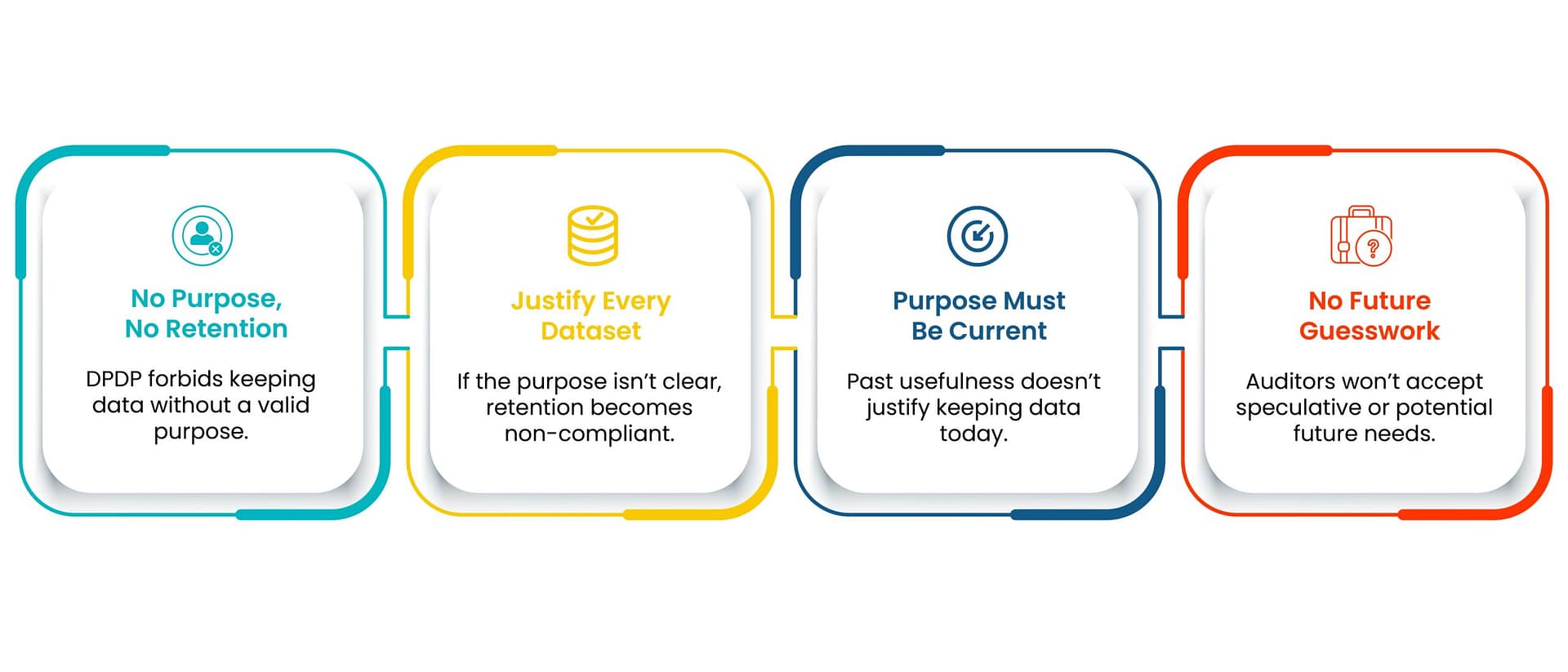 Channel level opt outs address only one symptom.
Channel level opt outs address only one symptom.